Contributors
Dr Sadashiv Baburao Tamagond
Consultant Cardiothoracic and Vascular Surgery

Dr M Pratyusha
Consultant CTVS Anesthesiologist
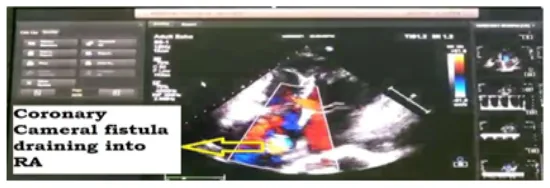
A 53-year-old female known case of hypertension presented with chest pain, palpitations, and progressive dyspnea on exertion for one year, ECG suggestive of Atrial Fibrillation, 2D Echo Findings (Fig1): suspicious RSOV shunt into RA, dilated RA, mild AR, normal systolic function. Coronary angiogram was suggestive of coronary Cameral Fistula from aneurysmal RCA to RA.

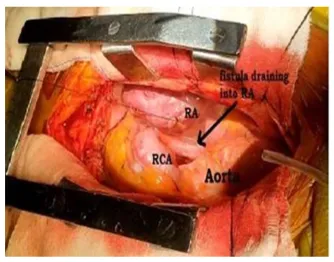
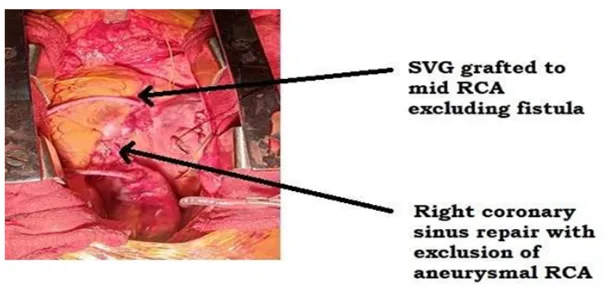
Operative finding: Coronary cameral fistula of 20mm size identified draining into RA at SVC junction (Fig3). Saphenous vein graft used for distal anastomosis to mid-RCA distal to aneurysmal segment. Following the aortic cross-clamp, an aortotomy has been performed. Left-side cardioplegia is given through left coronary ostia and right-side through vein graft for adequate myocardial protection. Aneurysmal dilated proximal RCA opened, and the ostium of mid-RCA was identified, closed with pledgeted suture excluded from the aneurysmal part; RCA is closed with a dacron patch and closed in double layer. The fistula opening in RA is closed with the pericardial patch (Fig 4). RA closed in layers. Weaned from cardiopulmonary bypass and decannulated.
The postoperative course in the hospital was uneventful, and the patient was discharged on the 5th postoperative day and is on regular follow-up.
Consultant Cardiothoracic and Vascular Surgery
Consultant CTVS Anesthesiologist

Click here to request a callback!