
A case of a diaphragmatic hernia.
Our patient is a 65-year-old lady who was presented with severe abdominal pain, vomiting, and difficulty breathing. Clinically, she had subacute intestinal obstruction.
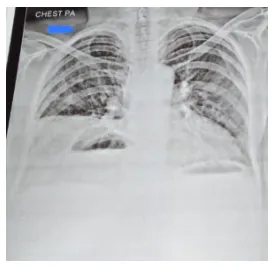
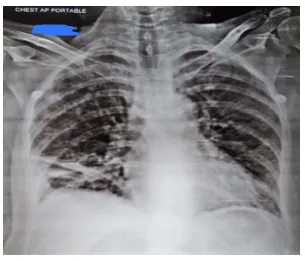
After admission and initial treatment, basic investigations were done. A routine chest X-ray suggested that there is a presence of bowel loops in the lower right thorax and elevated right dome of the diaphragm. This raised the suspicion of a diaphragmatic hernia, so the patient was subjected to HRCT thorax with CECT abdomen and pelvis. The CT scan confirmed that there was an elevation of the right side of the diaphragm with Morgagni’s type of diaphragmatic hernia. The left lobe of the liver, transverse colon, and stomach antrum was seen in the right lower thorax.
This confirmed the presence of a diaphragmatic hernia causing subacute intestinal obstruction. The patient was posted for diagnostic laparoscopy with the repair of a Diaphragmatic hernia.
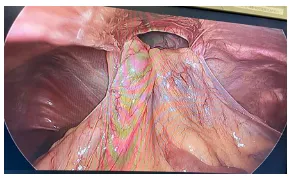
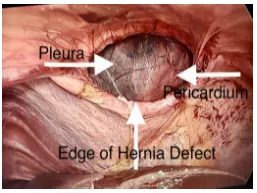
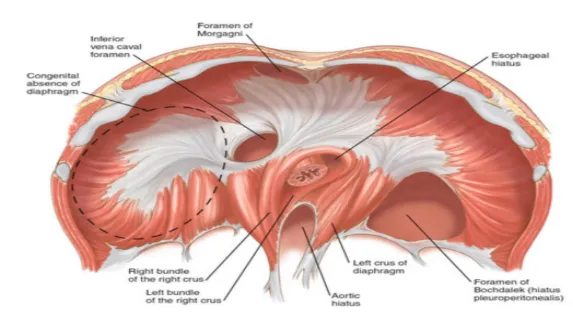
During surgery, the contents of the hernia sac, the stomach, the colon, and the left lobe of the liver, were reduced into the abdominal cavity. The falciform ligament was divided. The defect in the diaphragm was present anterior to the esophagus just behind the sternum, suggesting Morgagni’s hernia. The hernia defect was anatomically closed using intermittent sutures of 1-0 prolene.
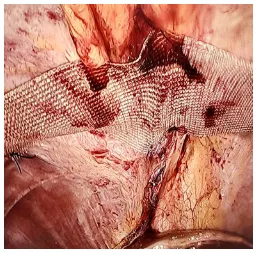
The repaired diaphragm was further reinforced using prolene mesh. The patient’s postoperative period was uneventful, and she was discharged on the third day after surgery.

Click here to request a callback!
