Contributors

Dr R Murarji
Consultant Pediatric Intensivist And Pediatrician
MBBS,MD Pediatrics
Fellowship In Pediatric Critical Care

A young patient was diagnosed with severe traumatic brain injury (TBI) accompanied by an extradural hematoma (EDH) and laryngomalacia. This story showcases the successful craniotomy and evacuation procedure that led to a remarkable recovery, underscoring the expertise and dedication of our medical team.
A seven-month-old male child was brought to Medicover Hospital in Kurnool on April 24th, 2024, around 8 AM, with an alleged history of falling from a bed at home. He had sustained a head injury, followed by excessive crying and vomiting, with altered sensorium occurring one hour after the injury.
The patient was taken to a different hospital where a CT-head was done, which showed an epidural hematoma (EDH) bleed. Later, the patient was referred to our hospital for further management.
At presentation to the hospital, the child was drowsy with GCS - E2V1M3 with a fall in O2 saturation. The child was immediately intubated and ventilated by our paediatric team. Neurosurgeon consultation was taken immediately, and the child was taken to OT within 15 minutes for surgery.
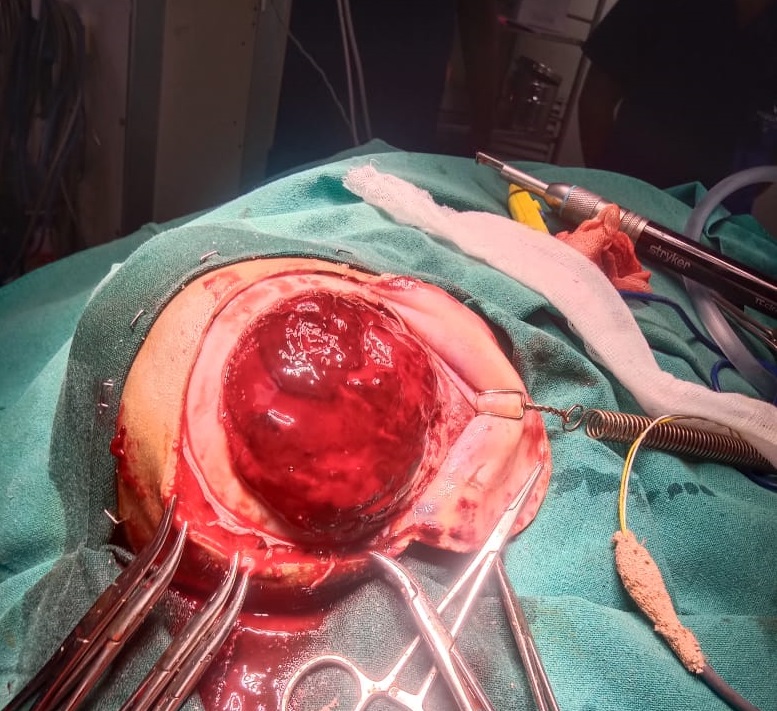
Later, the child has undergone craniotomy and evacuation of EDH (100 cc). In between, the kid was anaemic, hypotensive and had a cardiac arrest in the OT and was revived by giving one cycle of CPR with inotropic support.
Postoperatively, the child was kept on ventilator support with inotropic support, and antibiotics and antiepileptics were given as per protocols. The child regained consciousness the following day. The first attempt of extubation failed due to stridor, which developed due to laryngomalacia, and the child was reintubated with supportive medical management.
The child was extubated in the next two days. In POD1, the child was started on RT feeding and then normal feeding soon after extubation. The child recovered well and was discharged in good condition on the 10th day of hospitalisation i.e., on 3rd May, 2024. In the follow-up visit, the suture was removed, and the child developed good activity.
Our short operative time, early recognition of complications and management with team effort resulted in a successful outcome.

Consultant Pediatric Intensivist And Pediatrician
MBBS,MD Pediatrics
Fellowship In Pediatric Critical Care

Click here to request a callback!